Mothers-in-Law, Friends and Husbands: Leveraging Social Connections to Improve Women’s Reproductive Autonomy in India

In 2020, the World Health Organization reported that out of the 1.9 billion women of reproductive age (15-49 years) in the world, 1.1 billion women have a need for family planning. However, only 842 million women who report a need for family planning are using contraception, leaving 270 million women with an unmet need for contraception.
Unmet need for contraception can be attributed to various factors, ranging from physical barriers that women face to accessing family planning services to social stigma from communities and rigid cultural norms. As the demand for family planning and for contraception has increased in the past decade, to say that the lack of uptake in family planning is due solely to the lack of access to information about contraception would not only be simplistic but also ineffective in improving women’s reproductive autonomy.
When examining the constraints that women in patrilocal societies face from their households, a woman’s husband is typically identified as the primary reason for her limited decision-making capacity over her mobility and peer engagement. However, other household members may play an equally (if not more) important role in determining the intrahousehold power structures that dictates women’s reproductive choices, especially in contexts where extended families and more complex kinship structures within the household are prevalent.
Two new studies by Mahesh Karra and colleagues explore the role of women’s peer and social connections as a key determinant of their reproductive behavior and decision-making.
To date, Karra and co-authors have published two papers. While both studies focus on improving access to family planning for women, the first study, a World Bank Policy Research Working Paper, takes a double-pronged approach to test whether enabling women to visit a family planning clinic with a peer strengthens social ties as well as contraceptive use. The paper employed an intervention to provide women with vouchers to examine their impact on women’s social connections and healthcare-seeking behavior.
The second study, published in the American Economic Association (AEA) Papers and Proceedings (P&P), examines intrahousehold dynamics and the influence of household members over women’s reproductive choices. This study more deeply explores the role of the intervention specifically on Mother-in-Law (MILs) approval of family planning for her Daughter-in-Law (DILs).
Both studies have produced groundbreaking, novel findings that are policy-relevant and informative for programs.
A friend in need: The impact of the voucher intervention
According to the 2016 India National Family Health Survey (NFHS), one in five women in Uttar Pradesh reported having an unmet need for family planning, including in Jaunpur district, where fertility and unintended pregnancy are high. How does peer engagement help women to overcome household constraints and improve their reproductive autonomy? In the first study, Karra and colleagues conducted a randomized controlled trial in rural Jaunpur, Uttar Pradesh, the most populous state in India, to evaluate whether leveraging women’s social connections while also reducing the costs of family planning services could help women to overcome barriers to mobility and seek care.
Women in the study were recruited from settings where MILs are highly likely to resist their DILs use of family planning as much as (or even more so) than husbands. Karra and colleagues partnered with a local, private family planning clinic, the ADC Clinic in Chandwak. After conducting a baseline survey with women, the team randomly assigned women to either: 1) a control group; 2) a group of women who received a ‘Bring-A-Friend’ (BAF) voucher; or 3) a group of women who received an “Own” voucher. Both BAF and Own vouchers covered all family planning services at the ADC Clinic up to 2,000 rupees ($28) and were valid for a period of ten months. In addition:
- Women who received the BAF voucher were encouraged to bring along a peer other than their husband or MIL to accompany them to the ADC Clinic. The peers whom they brought could be anyone of their choosing, but women were encouraged to bring a peer who may also want to use family planning. Any peer who accompanied a woman to the ADC Clinic also received the voucher for subsidized family planning services over the ten-month period.
- Women who received the Own voucher received subsidized family planning services for their use only. This group was not explicitly encouraged to bring along a peer.
- Both treatment groups were offered reimbursement for transportation, for up to three visits to the clinic, which aimed to reduce transport barriers.
- All women in the study were revisited after ten months and were re-interviewed about their experiences with the intervention.
The researchers found that:
- Visits to the family planning clinic increased, as did the number of women who visited the clinic without their husbands or MILs.
- Modern contraceptive use increased by 56 percent, and this increase in uptake was more significant for women who reported that they had experienced social barriers, embarrassment, or a need for concealability when using contraceptives at baseline.
- Women in the BAF treatment group saw their number of close peers increase by 21 percent relative to the control group and the group that only received their own voucher.
- Women in the BAF group reported having lower levels of stigma towards family planning practices by 38 percent relative to women in the control group.
These findings have important implications for the effective implementation of policies and interventions that seek to improve outcomes for women in contexts where they lack access to care and have little say in their own health and reproductive decisions.
Overcoming barriers within the household: The approval of the Mummy-ji
In the AEA P&P study, Karra and coauthors explored the impact of the intervention on discussions around family planning between women and their MILs from the same study group as the World Bank study. The results highlighted a significant level of discordance in fertility and family planning preferences between MILs and DILs. This was found to be more glaring in the context of son preference, with MILs reporting wanting 1.4 more sons for their DILs than what DILs wanted, on average, as shown in Figure 1.
Figure 1: Misalignment in Fertility Preferences
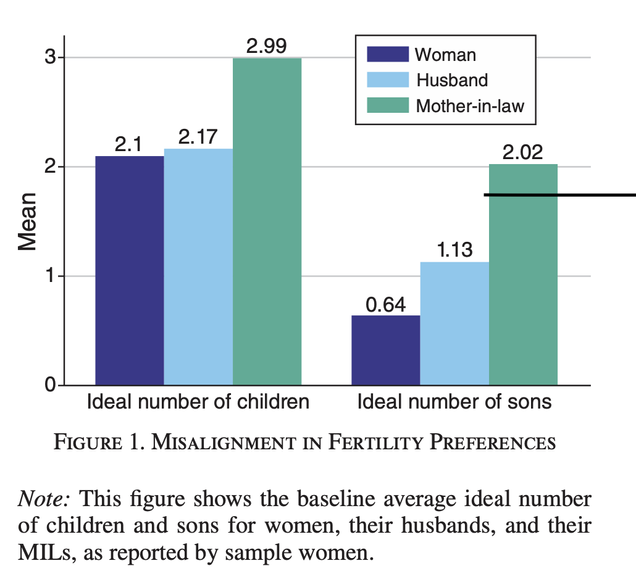
Source: Anukriti S., Herrera-Almanza C., Karra M., Valdebenito R. Convincing the Mummy-ji: Improving Mother-in-Law Approval of Family Planning in India. AEA Papers and Proceedings. 2022 May 1;112:568–72.
The researchers found that:
- MILs of DILs who received a voucher were between 8 to 11 percentage points more likely to approve of family planning for their DILs than women who did not receive a voucher.
- Women who received the voucher were also more likely to initiate conversations on contraception with their MILs.
- Women who received the voucher were also more likely to visit the family planning clinic.
While these findings suggest a higher rate of MIL approval of their DILs for family planning, the authors note that the results were driven mainly by women who did not have sons, which suggests that the voucher – which eased the burden of accessing family planning services – was useful in helping to overcome resistance from MILs.
The relevance of this study’s findings for similar settings within and outside India has a number of policy and programmatic implications of the role of household bargaining power through the lens of intergenerational gender attitudes. Programs that are designed to improve women’s access and autonomy – especially in family planning – must expand beyond socioeconomic barriers to consider the role of women’s mobility, social connectedness and household position.
Read the Bring-A-Friend Study Read the Mummy-ji Study*
Never miss an update: Subscribe to the Human Capital Initiative newsletter.