History of VR Development.
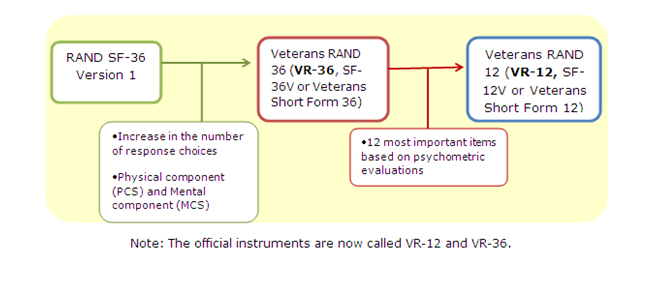
The VR-12© was developed from the Veterans RAND 36 Item Health Survey (VR-36©; formerly called the Veterans SF-36), which was adapted from the RAND 36-Item Health Survey (RAND 36 version 1.0) at the RAND Corporation and the Medical Outcomes Study. The VR-36© differs from the RAND 36 in the use of 5-point response choices for two of the eight scales, role limitations due to physical and emotional problems. Changes the yes/no choices for 7 of the items to 5-point response scale (“no, none of the time” to “yes, all of the time”) has resulted in a reduction to floor and ceiling effects of the scales with important gains to their distributional properties and increases to the reliability and validity of the assessments (Kazis et al 2004, Kazis et al 2006a, Kazis et al 2006b). The VR-36© eight domains include physical functioning, role limitations due to physical problems, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems and mental health. The eight scales are summarized into two summary scores, physical (PCS) and mental (MCS). With modifications in the VR-36©, the role scales have gained more than 80% in their reliability and 5% more precision for PCS and MCS summaries. The VR-36© and VR-12© also includes two “extra” items in order to assess how much physical and emotional health has changed over the past year. Validated conversion formulas have been developed for comparisons and bridges for VR-36© and VR-12© scores for studies that have used the RAND 36.
The VR-12© includes 12 items from the VR-36© and the 2 change items. The 12 items are a sampling of items from each of the eight domains of health from the VR-36©. The VR-12© explains 92% of the reliable variance of the VR-36©. Physical (PCS) and Mental (MCS) summary scores are computed based upon weights derived from the VR-36©. Each indicator variable is weighted for each of the response choices. The VR-12© computes comparable physical (PCS) and mental (MCS) summary scores to those in the RAND 36 and to those in the VR-36©. Differences reported are as small as 0.31 points for PCS and 0.06 points for MCS. The VR-12© has undergone extensive testing and shown to be reliable and valid in ambulatory care patient populations. Improvements to the VR-36©/VR-12© compared to the SF-36/SF-12 are also in the ability to detect change (Selim et al 2007, Selim et al 2010).
Bridges between the SF-36/SF-12/SF-6D and the VR-36©/VR-12©/VR-6D© PCS and MCS summary scores have been developed. Bridges between PROMIS and the VR-12© are currently under development.