Legislating to Build a Healthier World.
 About two weeks ago, we hosted a Public Health Forum featuring Cheryl Healton, dean of the College of Global Public Health at New York University. At the event, Healton discussed the Master Settlement Agreement (MSA), a 1998 agreement between 46 state’s attorneys general and the US tobacco industry. The MSA, which was the largest civil litigation settlement in US history, required tobacco companies to pay the states, through yearly installments, billions of dollars, as compensation for taxpayer money that had been spent as a consequence of tobacco-related diseases. The MSA also created restrictions for the marketing of cigarettes, with an eye toward reducing smoking, particularly among children. In this sense, the MSA was both a legal agreement and a tool for promoting health, demonstrating the power of the legal system to help create a healthier world. In the spirit of Healton’s talk, we today run a modified Dean’s Note on how the law can improve the health of the public, beginning with a look at how state and federal regulation shape issues of critical public health importance.
About two weeks ago, we hosted a Public Health Forum featuring Cheryl Healton, dean of the College of Global Public Health at New York University. At the event, Healton discussed the Master Settlement Agreement (MSA), a 1998 agreement between 46 state’s attorneys general and the US tobacco industry. The MSA, which was the largest civil litigation settlement in US history, required tobacco companies to pay the states, through yearly installments, billions of dollars, as compensation for taxpayer money that had been spent as a consequence of tobacco-related diseases. The MSA also created restrictions for the marketing of cigarettes, with an eye toward reducing smoking, particularly among children. In this sense, the MSA was both a legal agreement and a tool for promoting health, demonstrating the power of the legal system to help create a healthier world. In the spirit of Healton’s talk, we today run a modified Dean’s Note on how the law can improve the health of the public, beginning with a look at how state and federal regulation shape issues of critical public health importance.
Many public health powers are inherent state powers (also known as the state’s “police” and “parens patriae powers”): the Federal Government only has authority over health matters granted to it by the US Constitution—primarily through the government’s authority over foreign and interstate commerce and national defense, and its powers to impose taxes and spend the revenue. Federal powers, nonetheless, are much broader than they might appear to defenders of “states’ rights,” and have produced a fairly mature set of federal laws and agencies, responsible centrally for the promotion of health. The US Department of Health and Human Services (HHS) is an executive agency headed by the Secretary of Health and Human Services, and it oversees the National Institutes of Health, the Food and Drug Administration, the Centers for Disease Control and Prevention (CDC), the Office of the Surgeon General, as well as the Centers for Medicare & Medicaid (all programs and agencies authorized by Congress). Given the centrality of foundational conditions that also affect the health of the public, I would argue that federal agencies such as the Environmental Protection Agency, the National Highway Traffic Safety Administration, and the Department of Labor’s Occupational Safety and Health Administration, to name but a few, all take regular actions that are directly related to health, to say nothing of decisions made by a much broader range of other federal departments such as the Department of the Treasury. Indeed, it is hard to think of an agency that does not affect health.
For much of the twentieth century, public health practitioners were taught that states were the primary source of law governing health matters. Until the mid-1900s, public health work was concentrated in local health and environmental departments, where controlling contagious diseases and contaminated food and water in the community were the focus of the profession. Today, however, public health is a far more expansive, national and international field—one in which federal legislation and regulatory agencies provide the legal framework and substantial funding for meaningful public health programs. State and local public health programs still perform valuable core functions in providing services, but many of these (including surveillance, evaluation, Ryan White HIV treatment, and family planning services) would not exist in the absence of federal regulation and funding.
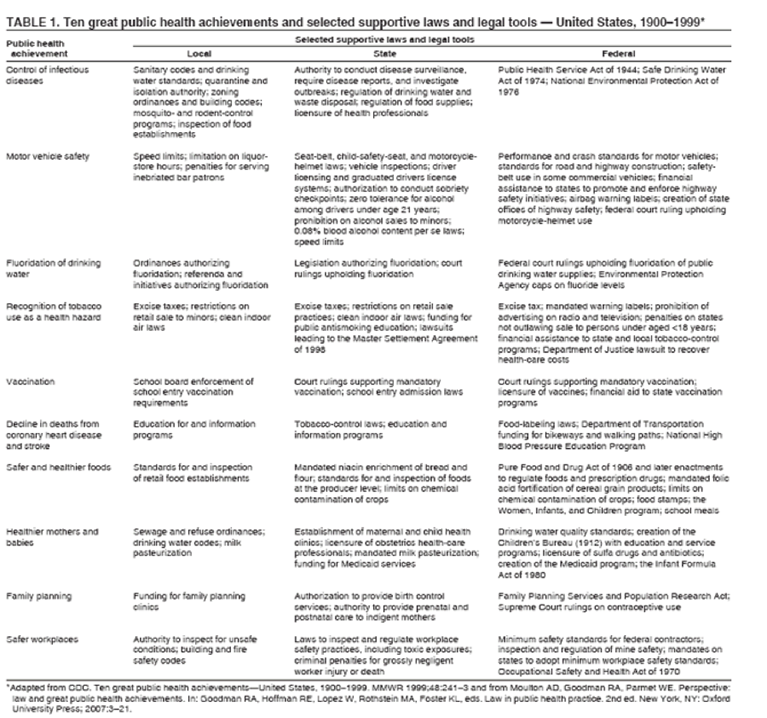
The observation that legal frameworks are supportive of, and necessary for, public health achievement is perhaps self-evident, but worth repeating. Figure 1 below shows how the ten great public health achievements, as articulated by the CDC, are all linked to respective supportive laws at the local, state and federal levels. Several authors have long written about the legal frameworks needed to deal with public health challenges such as the built environment and obesity. It goes almost without saying that health law scholars in our own school have contributed a substantial body of scholarship that informs our understanding of the intersection between laws and the health of populations.
At the same time, of course, we have, as previously discussed in many a Dean’s Note, substantially poorer achievement in health indicators as a country than many of our peer nations. All of which suggests, perhaps, that while we do indeed have legislation to promote particular aspects of health, we have far less legislation that aspires to promote population health through all our other regulatory and legislative efforts. Namely, while we have a mature set of laws that govern HHS, CDC and other health agencies, we are far from having health as a goal for the broad range of federal, state, and local laws that indeed shape the conditions that make people healthy.
Are there alternatives to this current state of affairs? In some respects, the progenitor of all public health regulation, the British Public Health Act of 1848, provided a prototype for how we may indeed improve public health by working on a range of sectors. It established both new laws about improving urban sanitary conditions, as well as formal public health infrastructures. The act was driven, perhaps idealistically, by the very particular concerns of its era. Coming right around the time of a major cholera outbreak, when acting to improve public health had become a pressing national imperative, the act established a general, central board of health, and in some places, local boards of health (where either a tenth or more of the taxpayers in the district petitioned the general board, or the death rate of the area exceeded the national death rate). The local boards were then tasked with dealing with issues such as water supplies and the removal of garbage and sewage. The act created positions for persons who were accountable for public health and penalties for noncompliance. In some ways, this measure was visionary in its focus on prevention and in establishing accountability for the health of the public. In reviewing the long-term impact of the act, Kenneth Calman well noted that its approach remains resonant and relevant today, but he wondered whether comparable acts could achieve traction in our time, given the challenges that assertive legislation aiming to improve public health has faced in the country. Perhaps ironically, the central driver for the act was maybe more economic than it was an aspiration towards healthier populations. Edwin Chadwick, the champion and namesake of this piece of legislation, knew that if he could improve the health of the poor, fewer people would seek relief from the government, ultimately saving money centrally.
Global examples provide some grounding about the scope of public health legislation that may have lessons for us in the domestic context. The Public Health Act in Northern Ireland was passed in 1967 to deal principally with infectious disease control, and was amended in 2008 to include the prevention of contamination by means of aircraft. The Quebec Public Health Act in 2002 affirmed the Minister of Health and Social Services’ authority to protect health, and passed specific legislation on vaccination registries, fluoridation of drinking water, infectious disease, and other crucial matters. Many similar public health acts have been passed around the world with the intention of clarifying the role of public health officials and allowing them to take immediate action for certain health hazards that present threats to the public. I note that often these acts take a rather traditional view of public health, targeting primarily infectious disease control. But there are exceptions that perhaps can motivate a more ambitious approach to the promotion of public health.
The Health in All Policies approach, first proposed in Europe nearly ten years ago, aspires to make health central to policy-making in all sectors of the economy. The approach recognizes that the production of health must arise from the engagement of multiple sectors, in order to create conditions for healthy populations. Other examples of Health in All Policies approaches include the Adelaide Statement in South Australia and ActNow BC in Canada. The Health in All Policies concept is also embedded in the Affordable Care Act, through the establishment of the National Prevention Council, under the direction of the Surgeon General, which has included the articulation of a National Prevention Strategy that lays out a framework for cross-sectoral action on health. The limitation of the latter, of course, is that it does not establish legislative ties to these actions, but rather acts to frame and nudge action by engaging multiple partners.
In sum, there is little doubt in my mind that legislative action stands to improve the health of the public. The challenge is that much of our conception of legislative actions for public health has focused on the specific regulation of public health (or health more broadly) taken by relevant agencies. While this is of course necessary, it is but a small piece of a much larger picture, and the need exists for a broader embrace of the social and structural changes required to promote health and prevent disease. In some ways, this is a call back to the roots of public health, as exemplified in the Public Health Act of 1848, echoed in more recent Health in All Policy Efforts. A recognition of the centrality of legislative efforts to the promotion of health, reflected in our school by work led through our Center for Health Law, Ethics, and Human Rights, is an essential component of our efforts to create healthy populations.
I hope everyone has a terrific week.
Warm regards,
Sandro
Sandro Galea, MD, DrPH
Dean and Robert A. Knox Professor
Boston University School of Public Health
Twitter: @sandrogalea
Acknowledgement: Thank you to Laura Sampson for her contributions to this Dean’s Note. I am particularly grateful to Professors George Annas and Wendy Mariner for inspiration, and for their substantive comments on earlier versions of this Dean’s Note.
Previous Dean’s Notes are archived at: https://www.bu.edu/sph/tag/deans-note/